
Table of Contents
⚠ Situation at a Glance as at 19 May 2026 (Cumulative)
Confirmed
Cases
51
Suspected
Cases
575
Suspected
Deaths
148
Countries
Affected
DRC &
Uganda
Confirmed
Deaths
4
- • PHEIC (Public Health Emergency of International Concern) declared by WHO Director-General: 17 May 2026.
- • NO approved vaccine or treatment exists for this Ebola strain.
1. Introduction and Background
1a. What Is Ebola
Ebola is a viral haemorrhagic fever, a very serious disease caused by a group of viruses called ebolaviruses. 'Haemorrhagic' means the disease can cause bleeding inside and outside the body. Ebola attacks many organs at once, breaking down the body's ability to control bleeding, fight infection, and keep its organs working. Ebola spreads from one person to another through contact with body fluids like blood, sweat, or vomit from a sick person. Without treatment, it can kill very quickly, sometimes within days. You cannot catch it through the air like a cold.
Think of it this way: if your body is a fortress, Ebola is an invader that sneaks in through the gates (your body's immune cells), then opens all the doors from the inside and destroys everything, the walls (blood vessels), the army (immune system), and the supply rooms (liver, kidneys, and spleen) — all at the same time.
1b. Some History
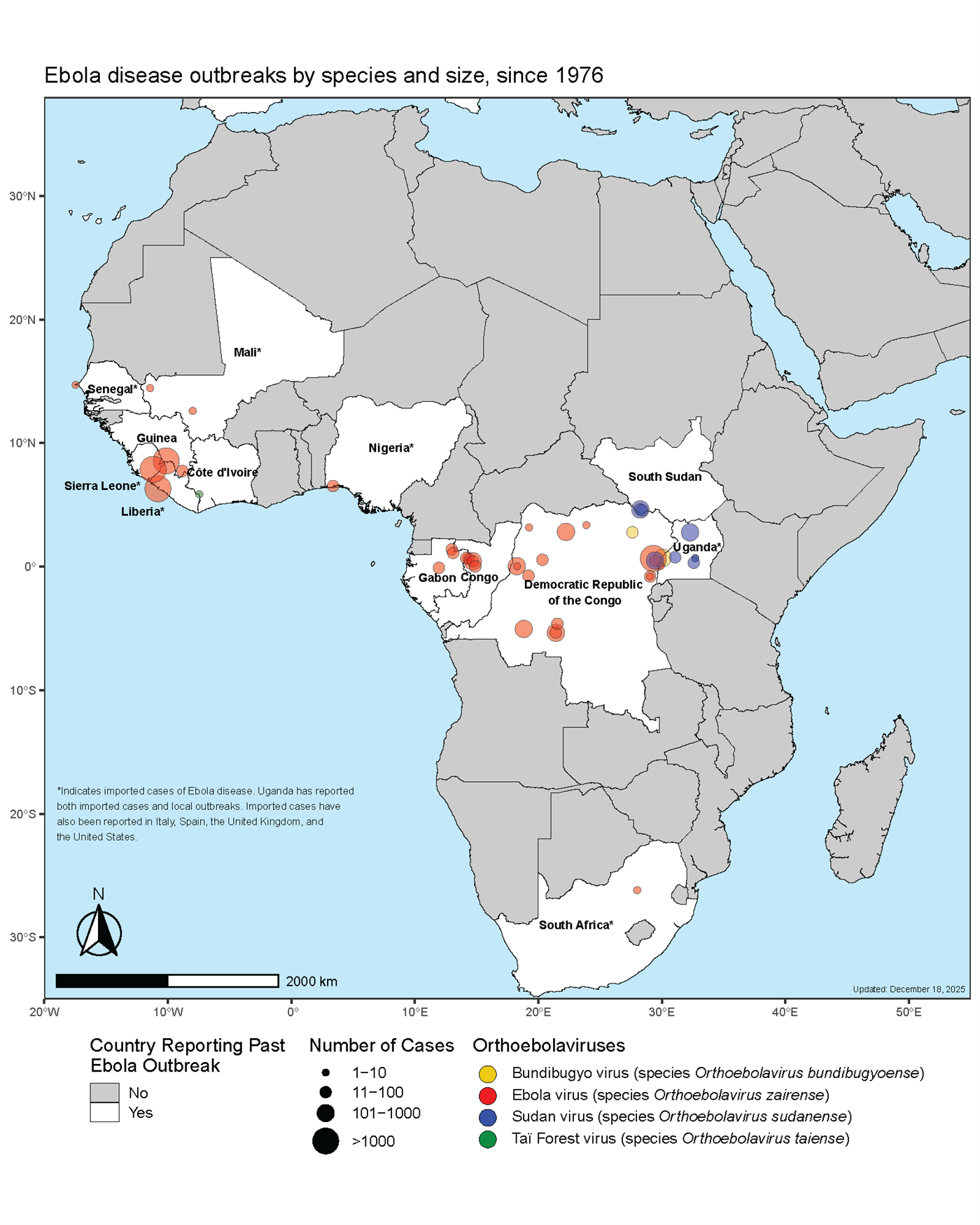
Ebola was first identified in 1976 in two simultaneous outbreaks in Central Africa: one near the Ebola River, Yambuku, DRC (then called Zaire which led to 318 cases, 280 deaths, Case Fatality Rate CFR ~ 90%) and one in Nzara, Sudan (284 cases, 151 deaths). Scientists named the virus after the Ebola River where the first outbreak was detected. Since then, Ebola has appeared in more than 40 documented outbreaks across Africa. The Democratic Republic of Congo (DRC) alone has experienced 17 outbreaks since 1976 – more than any country on Earth.
1c. The Five Known Ebola Virus Species
Scientists have identified five distinct species of ebolavirus, all belonging to the family Filoviridae and genus Ebolavirus. Three species cause major human outbreaks:
| Species | First Discovered | CFR | Vaccine? | Key Notes |
|---|---|---|---|---|
| Zaire ebolavirus (EBOV) | DRC, 1976 | Up to 90% | YES ✔ | Most outbreaks; 2014–2016 West Africa (28,600 cases) |
| Sudan ebolavirus (SUDV) | Sudan, 1976 | 41–70% | NO ✗ | Uganda 2022, 2025; several outbreaks in Sudan |
| Bundibugyo virus (BDBV) | Uganda, 2007 | 30–40% | NO ✗ | THIS OUTBREAK; only 3rd known occurrence |
| Taï Forest virus (TAFV) | Côte d'Ivoire, 1994 | Unknown | NO ✗ | Only 1 known human case (survived) |
| Reston ebolavirus (RESTV) | Philippines, 1989 | Not fatal | NO ✗ | Infects pigs; rare human exposure – no human deaths |
1d. Timeline of Recent Ebola Outbreaks in East & Central Africa (2022–2025)
- August 2022 – January 2023: Sudan ebolavirus outbreak in Uganda (Mubende); 142 confirmed cases, 55 deaths.
- August – December 2025: Zaire ebolavirus outbreak in DRC (Bulape, Kasai Province); 53 confirmed, 45 deaths. Outbreak declared over by authorities 1 December 2025.
- January – April 2025: Sudan ebolavirus outbreak in Uganda (Kampala/Mbale); 14 cases, declared over 26 April 2025.
- 15 May 2026: DRC confirms Bundibugyo ebolavirus outbreak in Ituri Province. Uganda confirms imported case same day. PHEIC declared 17 May 2026.
Source: Centers for Disease Control and Prevention. (Accessed May 17, 2026). Ebola outbreak history.
https://www.cdc.gov/ebola/outbreaks/index.html
2. The Bundibugyo Virus (BDBV)
2a. Biology of BDBV
The Bundibugyo virus (BDBV) is a negative-sense, single-stranded RNA virus that belongs to the family Filoviridae, genus Ebolavirus. The name 'filo' comes from the Latin word filum, meaning 'thread'. This is because under the microscope the virus looks like a long, twisted thread or worm rather than a round ball.
Here is what makes it special as a virus:
- It is TINY but complex: Its genome (genetic instruction book) is about 19 kilobases long and contains only 7 genes, each producing a specific protein the virus needs to survive and multiply.
- It has an envelope: The virus is wrapped in a fatty outer coat (envelope) taken from the cell it infected. This helps it hide from the body's immune system.
- Its most important weapon is the Glycoprotein (GP): This protein is like a 'key' on the surface of the virus that unlocks the door into human cells. Once inside, the virus uses the cell's own machinery to make millions of copies of itself.
- It attacks immune cells first: Ebola specifically targets macrophages (the body's 'patrol guards') and dendritic cells (the 'alarm-senders'). By attacking these first, the virus shuts down the body's early warning system before the main immune response can fire up.
2b. BDBV Reservoir
This is one of the most important and still unanswered questions in Ebola science.
🦇 The Bat Hypothesis (Current Best Scientific Thinking)
Fruit bats (family Pteropodidae), also called flying foxes, are the leading suspected reservoir host for ebolaviruses. Multiple studies have detected ebolavirus antibodies in African fruit bats, suggesting the animals have been exposed to the virus and survived. However – and this is very important – scientists have NEVER been able to isolate live Bundibugyo virus directly from a bat. The bat reservoir hypothesis is therefore scientifically strong but not 100% proven.
Other animals that may carry or transmit ebolaviruses to humans include: gorillas, chimpanzees, and duikers (small antelope). These are likely 'spillover' hosts — they get infected just like humans and can spread it further, but they are probably not the original source. Importantly, a 2024 experimental study (Lewis et al., 2024) showed that domestic pigs can be infected with BDBV and shed the virus, raising concern about more complex animal-to-human transmission pathways in farming communities.
2c. Transmission to Human Population (Zoonotic Spillover)
'Spillover' is the moment when a virus crosses from an animal into a human. For Bundibugyo and other ebolaviruses, this most likely happens through:
- Hunting and handling bushmeat: People who hunt, skin, or eat bats, primates, or other forest animals may come into contact with infected blood, organs, or tissue. In Ituri Province, bats are a common food source and are handled by hand.
- Eating forest fruits contaminated by bats: Bats often bite fruit and leave behind saliva or droppings. Humans who pick up and eat that fruit without washing it may ingest the virus.
- Mining activities: Miners in Ituri Province regularly enter deep forest areas and caves where bats live, increasing their exposure risk. The current outbreak epicentre includes Mongbwalu, a high-traffic gold mining area.
- Direct contact with bat roosts: Communities living near caves or large trees where bats roost may be exposed through contact with bat droppings, urine, or carcasses.
2d. How the Virus Spreads Between People (Human-to-Human Transmission)
Once the virus enters one person, it can spread to others, but ONLY through direct contact with body fluids of someone who is already showing symptoms. This includes:
- Blood, vomit, diarrhoea, sweat, saliva, urine, semen, and breast milk of a sick person.
- Touching or washing the body of someone who has died from Ebola (dead bodies remain highly infectious).
- Touching surfaces or materials (bedsheets, needles, gloves) contaminated with the body fluids of a sick person.
- Healthcare workers caring for patients without proper protective equipment (PPE) are at extremely high risk — as seen in the current outbreak where 4+ nurses and doctors have died.
Important: Ebola does NOT spread through the air like influenza or COVID-19, through water, or through casual contact like sitting next to someone, shaking hands, or sharing food with a healthy person. You cannot get it from a person who has the virus but has NOT yet shown symptoms (pre-symptomatic transmission is not confirmed for Ebola).
3. Epidemiology of the Current Outbreak: Bundibugyo Ebolavirus
3a. Key Epidemiological Facts About Bundibugyo Virus
Incubation Period
2 to 21 days (usually 6–7 days).
Case Fatality Rate (CFR)
30–40% in the two previous outbreaks (33.6% overall across 211 cases). This means roughly 1 in 3 infected people die. While lower than Zaire Ebola, it is still extremely high.
Vaccine or Treatment?
NO. Unlike Ebola Zaire, there are currently NO licensed vaccines or approved treatments for Bundibugyo virus. This is the single greatest challenge in the current outbreak.
3b. Pathogenesis of Bundibugyo
Understanding how the virus causes death helps explain why this disease is so serious and why certain public health measures are critical.
- The virus enters the body through mucous membranes (eyes, nose, mouth) or skin breaks and immediately begins infecting macrophages and dendritic cells — the very immune cells designed to destroy invaders.
- A 'cytokine storm' is triggered. Infected immune cells release large amounts of inflammatory chemicals called cytokines in a chaotic, disorganised burst. Instead of protecting the body, this storm causes widespread inflammation and tissue damage throughout the body.
- The liver is badly damaged. The liver produces the proteins that make blood clot normally. When BDBV destroys liver cells (hepatocellular necrosis), the body loses the ability to stop bleeding, leading to the haemorrhagic (bleeding) features of the disease.
- Blood vessels leak. The virus damages the inner lining of blood vessels (endothelium), making them 'leaky'. Fluid moves out of the bloodstream into surrounding tissues. This causes dangerous drops in blood pressure (shock) and organ failure.
- Multiple organs fail at once. The kidneys, spleen, adrenal glands, and other organs are attacked simultaneously. The body can no longer regulate fluid balance, blood pressure, or basic chemistry. Death typically occurs from hypovolemic shock (the body running out of functional blood volume) and multi-organ failure, usually between day 6 and day 16 of illness.
3c. Evolution of 2026 Ebola Outbreak: From Undetected Spread to Confirmed Diagnosis
The current outbreak almost certainly began in late April 2026 in Ituri Province, northeastern DRC, a region known for gold mining, armed conflict, dense forest, and high cross-border movement with Uganda and South Sudan.
- Late April to early May 2026: More deaths are reported in Mongbwalu and Rwampara health zones. Early samples were tested at Bunia's regional health centre using GeneXpert machines, but these machines are designed only to detect the Zaire strain, they returned FALSE NEGATIVE results. This made the outbreak spread undetected.
- 3–7 May 2026: Samples from Rwampara were sent to the INRB (National Institute of Biomedical Research) in Kinshasa. PCR tests capable of detecting multiple Ebola species were run and return POSITIVE for a non-Zaire ebolavirus.
- 15 May 2026: DRC Ministry of Health officially confirms Bundibugyo ebolavirus outbreak. More than 246 suspected cases and 80 deaths already reported across Bunia, Rwampara, and Mongbwalu health zones.
- 14–16 May 2026: A 59-year-old Congolese man was admitted to Kibuli Muslim Hospital in Kampala, Uganda on 11 May, died on the 14 May, and tests positive for BDBV (meaning he died before results proved positive). A second confirmed case was reported in Kampala on 16 May 2026. Both individuals had traveled from DRC. No evidence yet of local Ugandan-to-Ugandan transmission.
- 17 May 2026: Dr Tedros Adhanom Ghebreyesus, the WHO Director-General declares a Public Health Emergency of International Concern (PHEIC).
3d. PHEIC Declaration: What It Is and Why It Was Declared
🌍 Public Health Emergency of International Concern (PHEIC) — Declared 17 May 2026
A PHEIC is the highest level of global health alarm that the World Health Organization (WHO) can declare under international law (International Health Regulations, IHR 2005).
In one sentence: a PHEIC is an official warning to all countries that a disease event is serious, unusual, and has the potential to spread internationally; thus, the entire world must coordinate to prevent or stop it through evidence-based public health measures.
WHO declared PHEIC for the current outbreak because:
- The outbreak has spread to three health zones, reached both Kinshasa (DRC's capital) and Kampala (Uganda's capital) almost simultaneously.
- There are NO approved vaccines or treatments for Bundibugyo, giving health authorities very limited tools to fight it.
- The scale of the outbreak is almost certainly much larger than the confirmed numbers suggest.
- The affected region borders Uganda AND South Sudan, with very high population movement (mining, trade, refugees).
- Active armed conflict in eastern DRC severely limits the public health response.
What a PHEIC does: it gives WHO's Director-General legal authority to issue binding 'temporary recommendations' to all member countries, it mobilises emergency funding, and it elevates global political attention to the response.
4. Public Health Response Measures
The following measures are proven by decades of Ebola outbreak science to stop or slow transmission. There is an ongoing implementation of these for the current outbreak but with gaps:
4.1 Surveillance and Active Case Finding
Health teams conduct active, systematic searches for sick people in affected communities, going door-to-door and reviewing records from hospitals and health centres. Community health workers and volunteers are trained to identify and report anyone with fever or Ebola-like symptoms. In the current outbreak, community death surveillance is a specific priority, given that many deaths occurred before formal case detection.
4.2 Risk Communication and Community Engagement (RCCE)
Communities that distrust or misunderstand Ebola response measures can actively undermine them — hiding sick relatives, resisting burial protocols, or fleeing treatment centres and spreading the virus further. Evidence-based RCCE means delivering accurate, timely, culturally appropriate information through trusted community leaders, local radio, and community health workers. Simultaneously, authorities must listen to and address community fears and concerns, not simply broadcast instructions.
4.3 Contact Tracing
Every confirmed or suspected Ebola patient's recent contacts (family, healthcare workers, funeral attendees) are identified and monitored for 21 days, the maximum incubation period. If any contact develops symptoms, they are immediately isolated and tested. This 'chain-breaking' is how Ebola outbreaks are ultimately stopped. Gaps in contact listing have been specifically identified in the current outbreak and represent a major weakness that must be urgently addressed, particularly in areas affected by armed insecurity.
4.4 Isolation and Case Management
Any confirmed or suspected case is immediately isolated in a dedicated treatment unit to prevent further spread. Even without a specific Bundibugyo antiviral, high-quality supportive care significantly improves survival: intravenous fluids and electrolyte replacement to prevent dehydration; treating concurrent infections (malaria, typhoid); pain management; and careful monitoring of organ function.
4.5 Infection Prevention and Control (IPC) in Health Facilities
Healthcare facilities must implement strict safety protocols: full personal protective equipment (PPE) including gloves, gowns, face shields, and masks for all staff in contact with suspected cases; dedicated Ebola isolation wards; environmental decontamination; and safe disposal of medical waste. The death of at least four healthcare workers in the current outbreak signals dangerous IPC gaps in Ituri health facilities. Ebola routinely amplifies in hospitals when IPC is inadequate, as was seen in the 2018–2020 North Kivu epidemic.
4.6 Safe and Dignified Burials (SDB)
A body infected with Ebola remains highly contagious after death — sometimes more so than during life. Traditional funeral practices in eastern DRC and Uganda often involve washing, touching, and kissing the deceased. It is therefore important to engage communities, including religious leaders and traditional authorities to explain the scientific need for safe burials to prevent further spread and maintain community cooperation.
4.7 Laboratory Diagnostics
This outbreak was delayed in detection because field-level GeneXpert machines in Bunia were calibrated only for Ebola Zaire. An urgent priority is to deploy point-of-care tests capable of detecting Bundibugyo virus directly in Ituri Province. Currently, samples must travel ~1,000 km to Kinshasa's INRB for PCR confirmation – an unacceptable delay in a fast-moving outbreak. Whole genome sequencing is also critical to map transmission chains, detect mutations, and identify the likely zoonotic source.
4.8 Cross-Border Surveillance and Regional Coordination
With cases already confirmed in Kampala (Uganda) and concern about South Sudan, formal cross-border mechanisms are essential. Africa CDC has convened a high-level regional coordination meeting with DRC, Uganda, and South Sudan health ministries, WHO, UNICEF, and international partners. WHO recommends health screening at all major border crossings, rapid sharing of epidemiological data, and joint contact tracing for cross-border cases. Border closure is NOT recommended by WHO, as it drives unofficial crossings that are harder to monitor and undermines trust.
⚠ 4.9 Medical Countermeasures Research (Critical Gap)
For Ebola Zaire, two licensed vaccines (rVSV-ZEBOV / Ervebo; Ad26.ZEBOV, MVA-BN-Filo / Zabdeno-Mvabea) and two approved monoclonal antibody treatments (Inmazeb, Ebanga) exist. None of these work for Bundibugyo virus. Several experimental vaccines and antivirals are in early development pipelines, but none have completed clinical trials for BDBV. Accelerated emergency research programmes, supported by international funding mechanisms like CEPI (Coalition for Epidemic Preparedness Innovations), must be urgently activated.
5. Conclusions
The 2026 Ebola Bundibugyo outbreak in DRC and Uganda is a rare, rapidly evolving, and deeply concerning public health crisis. It is only the third time in recorded history that BDBV has caused a large human outbreak, and the first time this strain has spread to the capital cities of two countries simultaneously. The WHO PHEIC declaration on 17 May 2026 reflects both the extraordinary scale and the severe global risk this event poses.
Several structural weaknesses significantly complicated the early response: the absence of Bundibugyo-capable diagnostic tools at the district level allowed the outbreak to spread silently for approximately three weeks before detection; ongoing armed conflict in Ituri Province actively prevented health teams from accessing affected communities; and the complete absence of any approved vaccine or treatment leaves health authorities with no medical countermeasures beyond supportive care and containment.
At the same time, there are real strengths: the DRC has successfully contained 16 previous Ebola outbreaks and has deep national expertise and institutional structures. Uganda has strong outbreak response capacity built through repeated experience. International partnerships such as the WHO, Africa CDC, US CDC, UNICEF, and others — are mobilising rapidly. The window to control this outbreak is narrow. With sustained political commitment, adequate international funding, and strong community engagement, containment is achievable.
6. Recommendations
For National Governments (DRC, Uganda, South Sudan)
- Mandate emergency PPE supply and mandatory IPC training for ALL health workers in affected and at-risk zones, and implement zero-tolerance enforcement of hospital safety protocols to prevent further healthcare worker deaths.
- Activate formal cross-border coordination mechanisms between DRC, Uganda, and South Sudan including joint contact tracing protocols, shared epidemiological data platforms, and screening at all major road and river crossings.
- Engage armed groups and local authorities in affected conflict zones to negotiate humanitarian access for health teams, and ensure health worker security.
- Do not implement border closures or international travel bans, which drive unmonitored movement and undermine regional trust and cooperation, as recommended by WHO.
For Research Institutions and Scientists
- Urgently conduct ecological and virological field surveys in Ituri Province bat populations and wildlife to identify the probable zoonotic source and reduce future spillover risk.
- Investigate the susceptibility of domestic pigs to BDBV in high-risk communities and assess whether livestock may represent an underappreciated amplifying host in the transmission chain.
- Share data and findings openly and rapidly through platforms like PubMed, preprint servers, and WHO technical briefings to accelerate global scientific response.
For Communities
- Wash hands frequently with soap and water, especially after contact with sick people, animals, or their environments.
- Do NOT touch or wash the body of someone who has died, especially if they showed signs of Ebola. Allow trained safe burial teams to handle this safely and respectfully.
- If you or a family member develops fever, weakness, vomiting, or bleeding, go immediately to a health facility. Do not wait, and do not visit a traditional healer first.
- Avoid handling, killing, or eating bats, primates, or animals found sick or dead in the forest.
- Listen to and cooperate with health workers and government health authorities. Share information about sick community members; early reporting saves lives. Do not spread rumours.
7. Reference List
Africa Centres for Disease Control and Prevention. (2026, May 15). Africa CDC calls for urgent regional coordination following Ebola virus disease outbreak in Ituri Province, DRC, and imported Ebola Bundibugyo case reported by Uganda. Link
Center for Infectious Disease Research and Policy. (2026, May). New Ebola outbreak hits Democratic Republic of Congo. University of Minnesota. Link
Centers for Disease Control and Prevention. (Accessed May 17, 2026). Ebola outbreak history. U.S. Department of Health and Human Services. Link
Cori, A., Nedjati Gilani, G., McCabe, R., Nash, R., Skarp, J., Morgenstern, C., Hauck, K., Ferguson, N., van Elsland, S., & Imperial College London School of Public Health. (2026, May). Ebola outbreak 2026: Q&A with experts. Imperial College London. Link
Falasca, L., Agrati, C., Petrosillo, N., Di Caro, A., Capobianchi, M. R., Ippolito, G., & Piacentini, M. (2015). Molecular mechanisms of Ebola virus pathogenesis: focus on cell death. Cell Death & Differentiation, 22(8), 1250–1259.
Judson, S. D., Fischer, R., Judson, A., & Munster, V. J. (2016). Ecological contexts of index cases and spillover events of different ebolaviruses. PLoS Pathogens, 12(8), e1005780. Link
Lewis, C. E., Pinette, M. M., Lakin, S. M., Smith, G., Fisher, M., Moffat, E., ... & Pickering, B. S. (2024). Experimental infection of Bundibugyo virus in domestic swine leads to viral shedding with evidence of Intraspecies transmission. Transboundary and Emerging Diseases, 2024(1), 5350769. Link
MacNeil, A., Farnon, E. C., Wamala, J., Okware, S., Cannon, D. L., Reed, Z., ... & Rollin, P. E. (2010). Proportion of deaths and clinical features in Bundibugyo Ebola virus infection, Uganda. Emerging Infectious Diseases, 16(12), 1969. Link
Rougeron, V., Feldmann, H., Grard, G., Becker, S., & Leroy, E. M. (2015). Ebola and Marburg haemorrhagic fever. Journal of Clinical Virology, 64, 111–119. Link
Ryabchikova, E. I., & Price, B. B. (2004). Ebola and Marburg viruses: a view of infection using electron microscopy. Link
Umar, S. K., & Diggle, M. A. (2025). The Ebola virus–going beyond the bleeding edge. Journal of Medical Microbiology, 74(7), 001998. Link
Van Kerkhove, M. D., Bento, A. I., Mills, H. L., Ferguson, N. M., & Donnelly, C. A. (2015). A review of epidemiological parameters from Ebola outbreaks to inform early public health decision-making. Scientific Data, 2(1), 150019. Link
World Health Organization Regional Office for Africa. (Accessed May 16, 2026). Democratic Republic of the Congo confirms new Ebola outbreak, WHO scales up support. Link
World Health Organization. (2020). Ebola Virus Disease Democratic Republic of Congo: External Situation Report 82. Link
World Health Organization. (2025, April 24). Ebola disease [Fact sheet]. Link
World Health Organization. (2025, February 21). Disease outbreak news: Sudan virus disease — Uganda (DON 556). Link
World Organisation for Animal Health (WOAH). (2024). Ebola virus disease. Link
World Health Organization. (Accessed May 17, 2026). Epidemic of Ebola Disease caused by Bundibugyo virus in the Democratic Republic of the Congo and Uganda determined a public health emergency of international concern. Link